The information highlighted (if any) are the most recent updates for this brand.
Each sachet contains Ethyl Icosapentate 900 mg.
Nonproprietary name: Ethyl Icosapentate (INN: Icosapent).
Chemical name: Ethyl(5Z,8Z,11Z,14Z,17Z)-icosa-5,8,11,14,17-pentaenoate.
Molecular formula: C22H34O2.
Molecular weight: 330.50.
Ethyl icosapentate is a colorless to pale yellow, clear liquid. It has a faint, characteristic odor. It is miscible with ethanol (99.5), with acetic acid (100) and with hexane. It is practically insoluble in water and in ethylene glycol.
Excipients/Inactive Ingredients: Tocopherol, Gelatin, D-sorbitol, Concentrated glycerin, Ethyl parahydroxybenzoate, Propyl parahydroxybenzoate.
PHARMACOLOGY: Pharmacodynamics: Serum Lipid-lowering Effect: This drug significantly lowers serum total cholesterol and serum triglyceride in patients with hyperlipidemia.
This drug lowers blood lipid level in animals with hyperlipidemia induced by high-cholesterol diet (rats and rabbits), rats with hyperlipidemia induced by casein-containing diet or Triton and animals fed with normal feed (rats and hamsters).
In oral administration in rats, EPA content of lipoprotein is increased and elimination of lipoprotein from blood is promoted.
The effects such as inhibition of absorption of cholesterol from intestine, inhibition of activity of its biosynthesis in liver and promotion of its catabolism and excretion into bile are shown (rats).
The effects such as inhibition of absorption of triglyceride from intestine, inhibition of activity of its biosynthesis in liver and inhibition of its secretion from liver, and increase in plasma lipoprotein lipase (LPL) activity are shown (rats).
Antiplatelet Effect: This drug inhibits platelet aggregation by various aggregating agents and similarly reduces platelet adhesiveness in patients with various thrombotic and atherosclerotic diseases.
This drug is considered to increase EPA content of mainly platelet membrane phospholipid and competitively inhibit the metabolism of arachidonic acid from platelet membrane, thereby inhibiting the production of thromboxane A2 and inhibiting platelet aggregation.
This drug inhibits platelet aggregation by collagen (rabbits, ex vivo).
This drug inhibits platelet aggregation by collagen, ADP and arachidonic acid in rats, rabbits and humans (in vitro).
Production of prostacyclin-like substance in the wall of thoracic aorta in rats was not changed or increased.
Maintenance of Arterial Distensibility: This drug inhibits the decrease in distensibility of isolated aorta of rabbits fed with high-cholesterol feed and maintains the distensibility comparable to that of aorta of rabbits fed with normal feed.
This drug inhibits the increase in pulse wave velocity (PWV) in thoracic aorta and femoral artery of rabbits fed with high-cholesterol feed. The PWV values are largely at the same level as those in rabbits fed with normal feed.
This drug inhibits the reduction of density and elastin content of vascular smooth muscle cells and accumulation of free cholesterol in smooth muscles and inhibits the growth of intimal smooth muscle cells in aorta of rabbits fed with high-cholesterol feed.
Effects in Various Arterial Occlusive Disease Models: Oral administration inhibits sudden death associated with thrombus formation caused by intravenous injection of arachidonic acid (rats) and inhibits thrombus formation in thrombotic obstruction of arteriovenous shunt (rats) and ellagic acid-induced thrombus (rabbits). This drug also inhibits the progression of lauric acid-induced peripheral gangrene (rats).
CLINICAL STUDIES: Data of EPADEL 300 mg and 600 mg: "Moderate" or better global improvement was achieved in 47.5% (19/40) of the subjects in a clinical study in patients with hyperlipidemia.
Data of EPADEL 300 mg (for reference): Hyperlipidemia: In clinical studies including double-blind controlled studies, "improved" or better and "mild" or better global improvement of hyperlipidemia were achieved in 43.8% (163/372) and 68.0% (253/372) of the subjects, respectively.
In long-term studies (24 to 52 weeks), serum total cholesterol (values before administration were 220 mg/dL or higher in 137 subjects) decreased by 3% to 6% and serum triglyceride (values before administration were 150 mg/dL or higher in 97 subjects) by 14% to 20%. These effects were stable.
When EPADEL 300mg were administered immediately after meals at a dose of 900 mg twice daily (morning and evening) or at a dose of 600 mg thrice daily (morning, noon and evening) for 12 weeks in a double-blind controlled study in patients with high serum triglyceride (TG) values, the rates of change in serum TG at the last evaluation in the twice-daily administration (230 subjects; serum TG before administration, 256.7 mg/dL) and in the thrice-daily administration (224 subjects; serum TG before administration, 249.4 mg/dL) were -12.62% and -10.65%, respectively, showing the value below the predetermined non-inferiority margin of 10%, which confirmed the non-inferiority of efficacy (in rate of change in serum TG) of twice-daily administration to that of thrice-daily administration.
Post-marketing Survey: JELIS: Patients with hyperlipidemia who had already received dietary instruction, have 250 mg/dL or higher serum total cholesterol values and were considered to require treatment with HMG-CoA reductase inhibitors (including patients with accompanying stable ischemic heart disease) were randomly allocated to the combined use of HMG-CoA reductase inhibitor (10 mg/day of pravastatin or 5 mg/day of simvastatin) and 1800 mg/day of EPADEL or the treatment only with HMG-CoA reductase inhibitor (control group). In 18,645 patients (9,326 in the EPADEL and 9,319 in the control group) included in efficacy evaluation who were followed up for 4.6 years on average in un-blinded manner, cardiovascular events (sudden cardiac death, fatal or nonfatal myocardial infarction, angina unstable and cardiovascular reconstruction) were observed in 262 patients (2.8%) in the EPADEL group and 324 patients (3.5%) in the control group. Hazard ratio was 0.81 (95% confidence interval, 0.69 to 0.95, the same applies hereinafter), indicating a significant reduction in the EPADEL group. Cardiovascular death (sudden cardiac death or fatal myocardial infarction) was observed in 29 patients (0.3%) in the EPADEL group and 31 patients (0.3%) in the control group. Hazard ratio was 0.94 (0.57 to 1.56). All deaths were observed in 286 patients (3.1%) in the EPADEL group and 265 patients (2.8%) in the control group. Hazard ratio was 1.09 (0.92 to 1.28). No significant difference was observed in either event.
Pharmacokinetics: Plasma Concentration: In single-dose oral administration of 2700 mg* of EPADEL immediately after a meal in healthy adult males, the maximum plasma concentration was achieved approximately 6 hours after the administration.
In oral administration of EPADEL at a dose of 600 mg or 900 mg 3 times a day, immediately after every meal, on consecutive days for 4 weeks, plasma concentration reached a steady state about 1 week after the start of the administration.
The pharmacokinetics was similar in 8-day repeated oral administration of EPADEL immediately after meals at a dose of 900 mg twice daily (morning and evening) and at a dose of 600 mg thrice daily (morning, noon and evening). The plasma concentration was gradually increased with the number of days of administration and reached a steady state on Day 5 to Day 6 in both groups.
*: The approved maximum dose of EPADEL is 900 mg per time.
Excretion (for reference): When 14C-labeled EPA-E was orally administered in male rats, 2.7% was excreted in urine and 16.7% in feces within 168 hours after the administration.
Forty-four point four percent of radioactivity was excreted in exhaled air.
Toxicology: Preclinical Safety data: Non-clinical data reveal no special hazard for humans based on conventional studies of repeated dose toxicity, genotoxicity, carcinogenic potential, toxicity to reproduction, and safety pharmacology.
Hypertriglyceridemia; in case of hypercholesterolemia use as an adjunct with effective antihypercholesterolemia drug.
As an adjunct to maximally tolerated statin therapy to reduce the risk of myocardial infarction, stroke, coronary revascularization, and unstable angina requiring hospitalization in adult patients with elevated triglyceride (TG) levels (> 200 mg/dL) and established cardiovascular disease; Or diabetes mellitus and 2 or more additional risk factors for cardiovascular disease.
As an adjunct to diet to reduce TG levels in adult patients with severe (≥ 500 mg/dL) hypertriglyceridemia.
The usual adult dosage for oral use is 1 sachet (1 sachet contains 900 mg as ethyl icosapentate) twice daily (1800 mg daily) after meals immediately. However, in cases of abnormalities in triglyceride, the dose can be increased to 1 sachet per dosing, given 3 times a day (2700 mg daily) depending on the severity of the abnormalities.
There are no special recommendations. Treatment should be symptomatic.
EPADEL S900 is contraindicated in patients with hemorrhage such as hemophilia, capillary fragility, gastrointestinal ulcer, urinary tract hemorrhage, hemoptysis, vitreous hemorrhage etc. It may become difficult to stop hemorrhage.
Careful Administration: (EPADEL S900 should be administered with care in the following patients): Patients having menstruation; Patients with a bleeding tendency; Patients scheduled to undergo a surgery [in patients from previous texts, bleeding may be aggravated]; Patients being treated with anticoagulants or drugs that inhibit platelet aggregation (see Interactions).
Important Precautions: When using EPADEL S900 for hyperlipidemia, sufficient attention should be paid to the following points: The use of EPADEL S900 should be considered after performing sufficient tests to confirm hyperlipidemia.
Diet therapy, which is the basis of the treatment of hyperlipidemia, should be used before EPADEL S900. Moreover, exercise therapy or reduction of risk factors for ischemic heart disease such as hypertension and smoking should be sufficiently considered.
Blood lipid level should be measured regularly during the administration and if there is no response to the administration, the administration should be discontinued.
Precautions concerning Use: In oral administration: Because EPADEL S900 is not absorbed well when taken on an empty stomach, patients should be instructed to take it immediately after meals.
Patients should be instructed to take EPADEL S900 without chewing.
Other Precautions: Cerebral haemorrhage was reported in a patient with poorly controlled hypertension using other antiplatelet drugs concomitantly.
Effects on ability to drive and use machine: Effects on ability to drive and use machines have not been studied.
Use in Children: Safety in low birth weight infants, neonates, infants and children has not been established (there is no clinical experience).
Because safety in the use during pregnancy has not been established, EPADEL S900 should only be administered when therapeutic benefit is judged to outweigh the risk in women who are or may be pregnant.
It is desirable not to administer EPADEL S900 in lactating women. When it is administered for compelling reasons, breastfeeding should be avoided. (Excretion into breast milk has been reported in animal studies [rats].)
In the clinical studies in patients with arteriosclerosis obliterans and hyperlipidemia in Japan and the postmarketing drug use-results survey, adverse reactions were observed in 647 of 14,605 patients who used EPADEL (4.4%) (at the time of completion of reexamination).
In double-blind controlled study in patients with high serum triglyceride, adverse reactions were observed in 9 of 241 subjects (3.7%) in twice-daily administration of 900 mg and 9 of 235 subjects (3.8%) in administration of 600 mg 3 times a day (at the time of approval of additional dosage and administration).
Clinically significant adverse reactions: Hepatic function disorder, jaundice (incidence unknown).
Patients should be closely observed because hepatic function disorder and jaundice with increased AST (GOT), ALT (GPT), Al-P, γ-GTP, LDH, bilirubin, etc may occur. If any abnormality is observed, the administration should be immediately discontinued and appropriate measures should be taken.
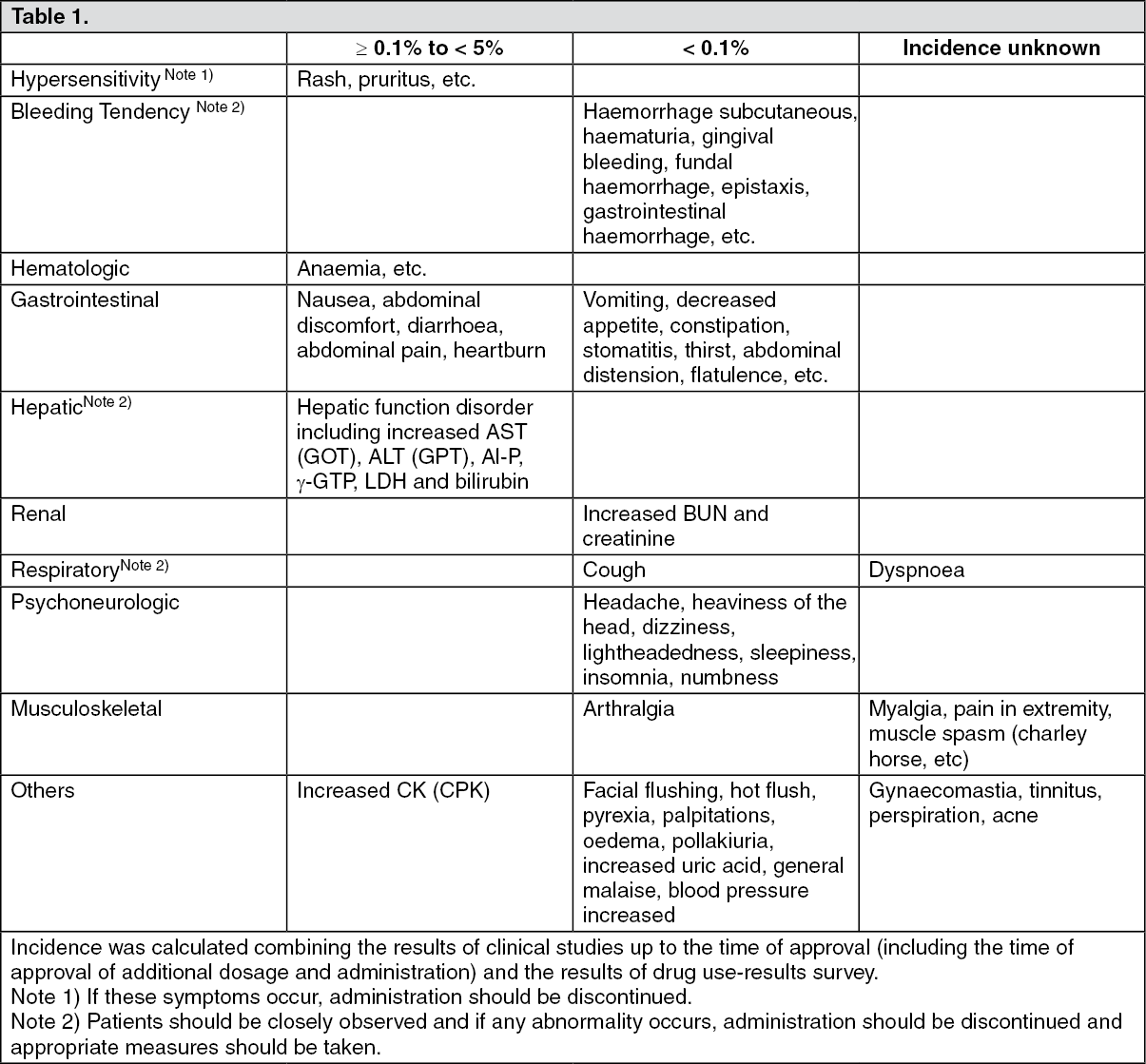
Other adverse reactions: If the following adverse reactions occur, appropriate measures should be taken according to symptoms. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Precaution for Coadministration (EPADEL S900) should be administered with care when coadministered with the following drugs: See Table 2.
Click on icon to see table/diagram/image
Incompatibilities: Not applicable.
C10AX06 - omega-3-triglycerides incl. other esters and acids ; Belongs to the class of other lipid modifying agents.
Epadel S900 soft cap 900 mg
84 × 45's




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
